Trigger warning: discussion of suicide and its depictions.
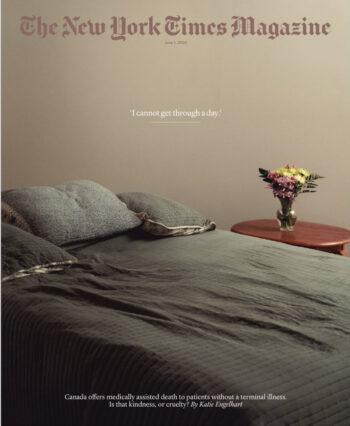
The New York Times Magazine (6/1/25) ignored ethical guidelines designed to keep reporting from encouraging suicide.
The New York Times Magazine recently published a cover story (6/1/25) that gave in-depth representation to the challenges faced by a chronically sick, disabled woman named Paula Ritchie, age 52. Ritchie dealt with underdiagnosed illnesses and pain, as well as challenges in supporting herself and managing her mental health.
The Times then told the story of Ritchie ending her own life out of despair over her situation. The journalist, Katie Engelhart, observed and documented her suicide, up until the last breath left her body. “I was with Ritchie until the very end,” she posted on X (6/1/25). Engelhart gave lengthy justifications for Ritchie’s choice to end her life, and described several people who supported her in that decision.
Articles like this aren’t common in the media. Suicide prevention is typically regarded as both a social good and an ethical responsibility. In the US and Canada (where the article takes place), suicidal people are involuntarily detained to prevent their deaths. It has long been illegal in Canada (and many US states) to assist or even “counsel” a person to commit suicide.
There are also ethical standards that guide media outlets in reporting on suicide, in order to minimize the risk of glamorizing or idealizing it. These guidelines are based on research showing that the media has an outsized influence when it comes to suicide. Graphic, detailed and sensationalized coverage has been shown to increase the “risk of contagion,” according to one guide. AP News specifically tries to avoid detailing the “methods used” in stories that reference suicide, based on this research.
The Times violated almost all of the published guidelines by personalizing, detailing, dramatizing, justifying and sentimentalizing Ritchie’s suicide, as well as by making it a cover story. The story featured close-up images of the method of Ritchie’s death and what appears to be her post-mortem body.
The World Health Organization urges journalists covering suicide not to “explicitly describe the method used” or “use photographs, video footage or social media links that relate to the circumstances of the suicide,” among other guidelines.
So why wasn’t there generalized outrage or pushback from other media? The only significant outcry came from thousands of disabled people on social media.
The simplest answer is that Ritchie’s suicide was administered by a doctor, and legal in Canada. Media tend to be more accepting of the unacceptable when it is government-sanctioned. In 2021, the country expanded its Medical Assistance in Dying (MAiD) law to permit physician-assisted suicide for disabled people who aren’t suffering terminal illnesses. The law and its implementation have been extremely controversial, as the article noted. Similar laws have been passed or introduced across Europe.
The Times article reinforced a popular belief that disability is a fate worse than death. The disabled author Imani Barbarin sums it up in the title of her forthcoming book: If I Were You, I’d Kill Myself. It’s a refrain disabled people are accustomed to hearing, the frightful implication of which is that accommodations aren’t worth the bother, and death is for their own good.
The media has a tendency to reinforce this idea in stories about disability. As I previously wrote about for FAIR (1/20/21), the New York Times (4/10/20, 12/24/20) published stories early in the Covid-19 pandemic suggesting that disability should be considered in determining who had a right to Covid ventilators, based on unproven myths of “quality of life.” The articles cited literal eugenicists as experts, and didn’t invite disabled people to the conversation.
Both sides, and propaganda
In Engelhart’s Times article, she appeared to offer a sensitive and balanced view on the debates around MAiD expansion. Yet the article was laden with ableist rhetoric, medical misinformation and subtle propaganda from the well-funded “right to die” movement. It also left out prominent critical facts about MAiD.
Engelhart omitted that the United Nations Convention on the Rights of Persons with Disabilities (3/11/25) issued a report in March that condemned Canada’s MAiD, and recommended that the country “repeal” the expanded law and halt plans for future expansion. The report outlined how benefits and healthcare for disabled people are inadequate in Canada, resulting in coercion around MAiD, especially for women and marginalized groups. People have been sharing stories of coercive MAiD practices since it was expanded (e.g., Independent, 6/23/23; New York Post, 11/8/22; X, 6/4/25).
It’s significant that the most powerful international body issued such a strong condemnation of MAiD; it’s something that anyone following the issue should know about, and Engelhart has published a book on MAiD and speaks about it constantly, yet she left it out of her article.

Dying With Dignity Canada’s goals include, according to the Walrus (1/12/24) “making MAiD available to people whose sole condition is a mental disorder” and “expanding MAID to ‘mature minors’ age twelve and older.”
Engelhart did discuss some of the issues exposed by the UN, but she cited “disability rights advocates,” “critics” and “opponents,” not the UN. She also didn’t name or quote these opponents, aside from a few uneasy doctors. None of the many disability rights, human rights and religious organizations that have condemned MAiD expansion were named, and only some of their arguments were discussed. Missing, for instance, was the fact that a promised expansion of disability benefits was tabled just after MAiD expansion was approved, suggesting the government saw the suicide program as another solution, of sorts, to the disability problem.
Also missing from the article was the role of a powerful lobbying group known as Dying with Dignity Canada (DwD), which has raised millions of dollars from corporate and wealthy donors (Walrus, 1/12/24). DwD has had an enormous influence on the Canadian government and media conversations on MAiD. The organization isn’t named in the Times Magazine piece, but its propaganda is subtly woven throughout.
Engelhart has been more explicit about her pro-MAiD leanings in other writings and statements (e.g., Neiman Storyboard, 3/3/21; NPR, 3/9/21), as well as in online responses to comments on her Times Magazine piece.
In search of euphemism
As evidence of her bias, look at the way Engelhart introduced the terminology in the Times article: “Canada’s Medical Assistance in Dying (MAiD) program—what critics call physician-assisted suicide.” It’s a curious attribution. Is there a more direct, factual way to describe what happened to Ritchie than suicide? It’s a subtle nod to DwD, which seeks to remove the “suicide” from assisted suicide. From the organization’s website:
We do not use the terms assisted suicide or euthanasia because they stigmatize people who are suffering intolerably and want to access their right to a peaceful death. Suicide is a desperate act of self-harm, while medical assistance in dying is a legal, federally regulated end-of-life choice, driven by hope and autonomy.
The Merriam-Webster definition of suicide is “the act or an instance of ending one’s own life voluntarily and intentionally.” DwD seems to be attempting to redefine the word to soften what happens with MAiD.
On Twitter, Engelhart has argued that “assisted death” is a less “politically loaded” term than “assisted suicide.” She has also taken issue with the AP for referring to MAiD recipients as “killed.” It’s not propaganda to state that when someone dies, they are “killed” by the cause of death. People are killed by cancer, accidents and self-inflicted wounds as much as by murder.
Engelhart’s efforts to soften the language of assisted suicide calls to mind crime reporters using “police-involved shooting” to say that police have shot someone. The common norms for speaking about suicide and shootings can apply without harm or distortion of the facts.
The Times Magazine article reflected some of the contradictions inherent to DwD ideology that appear throughout Engelhart’s work. For instance, she often compares assisted suicide rights to abortion rights, a DwD talking point. But she also compares it to the merciful “euthanizing” of “beloved pets.” Unlike people who elect abortions, animals do not get to choose their fates, or even express their wishes. Humans project our assumptions onto pets, including that their suffering must be a fate worse than death.
Despite Engelhart’s seeming alignment with the “dying with dignity” movement, to her credit, she did expose that there wasn’t absolute “dignity” in Ritchie’s death. The article ends with a gruesome description of Ritchie’s last moments, including her expression of “horrible” discomfort.
A ‘difficult case’

Dr. Matt Wonnacott, the doctor who approved euthanasia for Paula Ritchie: “If you tell me that you’re suffering, who am I to question that?” he told Engelhart.
Engelhart provided a lot of detail about Ritchie’s medical conditions, but relied on outdated, vaguely sourced and ableist ways of describing chronic illness. Here and elsewhere, her work is mostly sourced to doctors, especially MAiD providers, and patients who want to die, but not the many people who live with and manage complex chronic disease.
As a disabled journalist, I see Ritchie’s story through a different lens than Engelhart. I have many of her conditions, deal with ongoing suffering, sometimes severe, and was suicidal at one point.
Engelhart described Ritchie as if she were too difficult to diagnose sufficiently beyond a collection of symptoms, including head injury, migraine, fatigue, dizziness, long-standing depression and PTSD from childhood trauma. Yet I know that it can take ten or more years for a person to get properly diagnosed with most chronic illnesses, if they are lucky. I also know that chronic illness patients deal with doctors who gaslight, misdiagnose and psychologize symptoms.
The doctor who authorized Ritchie’s suicide, Matt Wonnacott, appears to be one of those. He was a primary source in the story. Engelhart did leave it open for readers to feel uncomfortable with Wonnacott’s approach. Although he acknowledged that Ritchie still had treatment options, he admitted to making decisions to approve assisted suicide based on “gestalt” and “patient choice” more than medicine. On the other hand, Engelhart seemed to take the doctor’s medical assessments at face value, not interrogating his knowledge or biases.
At one point, Engelhart referred to a category of MAiD patients with “functional disorders…that are poorly understood within medicine, and disputed within medicine, and that some clinicians believe have a significant psychological component.” Who are these clinicians? She did not say, but then listed a series of conditions that are not considered, by official diagnostic criteria, to be psychological: “fibromyalgia, chronic fatigue, irritable-bowel syndrome, some kinds of chronic headaches.” “Functional” has a history, like “hysteria” before it, of being used as a catch-all for misunderstood women’s illnesses.
As for “chronic fatigue,” it is more properly known as Myalgic Encephalomyelitis, or ME. There is an epidemic of it lately, as it is commonly caused by Covid-19. As such, there are countless recent studies proving its physiological causes. At one point, Engelhart discussed how Ritchie’s muscles work one minute, then “suddenly buckle” the next, writing: “This suggested that the buckling was due to psychological causes or a lack of effort.” Yet Ritchie seemed to be demonstrating a hallmark symptom of ME known as “post-exertional malaise.”
Engelhart included a lot of detail about Ritchie’s care and medications, with the effect of seeming like every option was exhausted. Yet I am surprised by what is missing. There is no mention of dysautonomia or its treatments, even though Ritchie has difficulty bathing herself and getting out of the bath, both common in that illness. There is no mention of cutting-edge treatments for ME, like antivirals for reactivated viruses, or naltrexone. And there is no mention of the new class of CGRP migraine drugs, which have rescued millions of people from horrible constant pain.
In place of medical investigation, Engelhart uses rhetoric and sentiment to portray Ritchie as a lost cause. She supports this portrait with classist and ableist imagery, like mentioning Ritchie’s “old TV and a window that looked out on a row of garbage bins,” her “stained” floors, her trouble bathing and long history of depression. She quotes people in Ritchie’s life who liked her, but also found her difficult, “vicious,” and “loud and excessive.”
I have a different perspective on Ritchie. She comes across to me as resourceful in pursuing help, a strong person who has survived tremendous suffering, and compassionate to others. She is surrounded by friends when she dies. She has common illnesses that have been under-researched due to medical misogyny. And she has been denied cutting-edge treatments due to the profound gulf between research and practice, as well as long-established bigotry in medical care. In my perception, if she had been properly diagnosed and treated, she may or may not have felt differently about ending her life.
Fly on the wall

The Economist‘s cover story (11/21/24) seemed to encourage not just legalizing suicide, but suicide itself.
Engelhart did a skillful job of portraying her own role in Ritchie’s suicide as if she were a passive observer. In a separate interview she gave with the Times about writing the piece, she said she “was trying to be as small a presence as possible in the room.” Yet she also admitted that Ritchie reached for her hand just before she died, so she couldn’t have been that small. Engelhart didn’t reflect, in the interview, on the role she may have played in Ritchie’s fate, or the ethics of her project.
The article emphasized that Ritchie knew she was being interviewed by a writer for the New York Times Magazine. She knew that her story would be amplified worldwide, but especially if she continued to end her life. Engelhart’s body of work on MAiD is mostly about people who elect and complete the act of suicide. That validation, alone, could have been a form of encouragement, especially for someone who felt isolated and unheard.
Best practices in suicide prevention are based on studies showing that suicidal people are uniquely and extremely vulnerable to suggestion, and that suicidality is usually temporary. According to a journalism guide from the Trevor Project, which aims to prevent suicide in LGBTQ youth, “More than 50 research studies worldwide have found that certain types of news coverage can increase the likelihood of suicide in vulnerable individuals.”
With the Times’ story, the worst-case scenario almost happened. One reader, a patient with Long Covid, responded on social media that the article caused him to consider that maybe assisted suicide would be a good option for him. After reading the responses of disabled people, he had more context and changed his mind. (I am protecting his identity.)
There is growing support for the expansion of assisted suicide across the world and in the media (e.g., Economist, 11/13/21, 11/21/24). The pandemic has eased people’s discomfort with preventable death, especially of elderly and disabled people. Engelhart’s book got a lot of attention around the height of Covid-19’s Omicron wave. Meanwhile, the current US administration is suggesting that worthiness for healthcare should be tied to social value.
It’s a key time for news organizations to recall their ethical obligations around reporting on suicide. At the very least, the news shouldn’t stop calling it “suicide” just because those who die have been approved for MAiD due to disability.
Stories of chronically sick people who resist MAiD and/or survive suicide attempts are rarely given as much in-depth treatment or column inches in the media. But those stories might give readers more context in considering how to feel about these policies. The New York Times even gave a flattering interview (11/16/24) to a doctor who has elsewhere been condemned for her unethical and too-eager MAiD practices and has been restricted from practicing everywhere (London Times, 7/19/24; Globe and Mail, 3/9/16).
News outlets should also consider hiring disabled journalists and editors to work on stories like this, or at least journalists who are curious enough to investigate medicine critically. Mainstream writing about health and disability has long ignored the insights of chronic illness patients, unless to use individual cases to speak over collective concerns. We need stories about disability and illness that don’t rely mostly on the medical establishment for expertise, especially given its long history of aligning with eugenics.
This content originally appeared on FAIR and was authored by Justine Barron.